
About MLD Support
MLD Support Association UK was set up to bring hope to families in the fight to eradicate Metachromatic Leukodystrophy (MLD).
Their main aim is to support families and sufferers of MLD by way of shared information from people in similar circumstances who have already experienced the effects of the condition and/or any treatments available. Their secondary aim to support research into therapeutic treatments for the condition through research grants to bona fide institutes engaged in such projects.
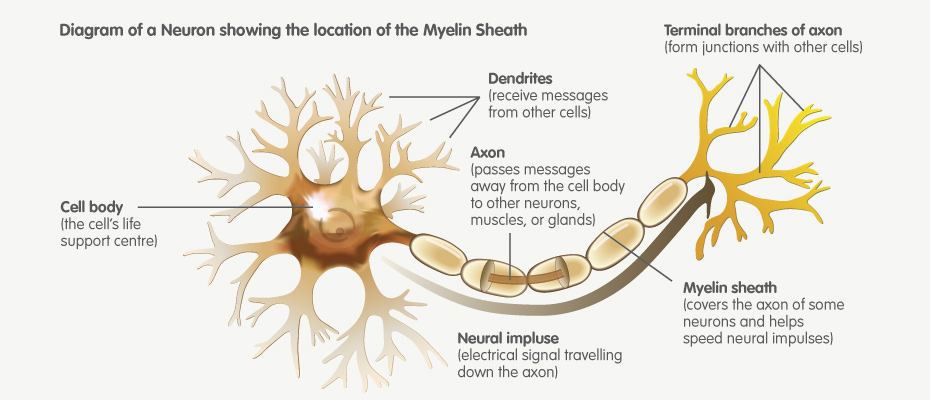
MLD is an acronym for Metachromatic Leukodystrophy. MLD is a genetic disorder which at the moment has no cure. MLD is directly caused by a deficiency of the enzyme Arylsulfatase A and is usually characterized by enzyme activity which is less than 10% of human controls. Without this enzyme, sulfatides build up in many tissues of the body, eventually destroying the myelin sheath of the nervous system. The myelin sheath is a fatty covering that protects nerve fibres. Without it, the nerves in the brain (central nervous system — CNS) and the peripheral nerves (peripheral nervous system — PNS) which control, among other things the muscles related to mobility, cease to function properly.
Building an economic model
I was asked by MLD to create an economic model which calculated and could provide evidence as to the potential cost and wider economic implications of the illness.
The mode it was envisaged would help to:
- To support the work of MLD by creating a robust model they can quote to clients, families, policy makers and the public
- To raise awareness of the impact of MLD
- Create a cost benefit analysis model for MLD
- Understand these costs relative to the cost of testing
- Account for the likelihood of MLD occurring
- Outline and use robust data sources
- Outline future challenges for MLD
To do this I not only had to consider the variables involved in treating such and illness, but also the probability of infection within the population and the various types and life expectancies of the illness. Broadly speaking MLD occurs in three forms:
Late Infantile MLD
In the late infantile form, which is the most common form of MLD (50-60%), affected children begin having difficulty walking after the first year of life, usually at 15–24 months. Symptoms include muscle wasting and weakness, muscle rigidity, developmental delays, progressive loss of vision leading to blindness, convulsions, impaired swallowing, paralysis, and dementia. Children may become comatose. Untreated, most children with this form of MLD die by age 5, often much sooner.
Juvenile MLD
Children with the juvenile form of MLD (onset between 3 and 10 years of age) usually begin with impaired school performance, mental deterioration, and dementia and then develop symptoms similar to the late infantile form but with slower progression. Age of death is variable, but normally within 10 to 15 years of symptom onset although some juveniles can live for several decades or longer after onset.
Adult-Onset MLD
The adult form of MLD commonly begins after age 16 and, in the initial stages, is often mis-diagnosed as a psychiatric disorder because of personality changes. Initially, the symptoms are cognitive rather than physical, then leading to progressive dementia and, ultimately, physical disability as well. Adult-onset MLD progresses more slowly than the late infantile and juvenile forms, with a protracted course of a decade or more.
The initial model
Within the initial model created for the charity were the following aspects:
- Cost of carer per hour
- Average number of hours care
- Lost earnings
- Probability of illness and average lifespan
- Investigation costs
- Medication costs
- Consultation costs
- Hospitalisation costs
- Special educational needs cost
- Additional travel costs
- Model across all three types of illness
Further developments
Further developments that could be made in the future were also identified and are as follows:
- Analysis of benefits/government support
- Reduction in illness rates due to sufficient testing
- Economic savings from sufficient testing
- Testing vs non testing scenario
- Psychological cost to patient
- The cost of raising awareness
- Future medical costs
www.mldsupportuk.org.uk